Cartographers Of Uncharted Waters - An Invitation To The Voyage
Free Chapter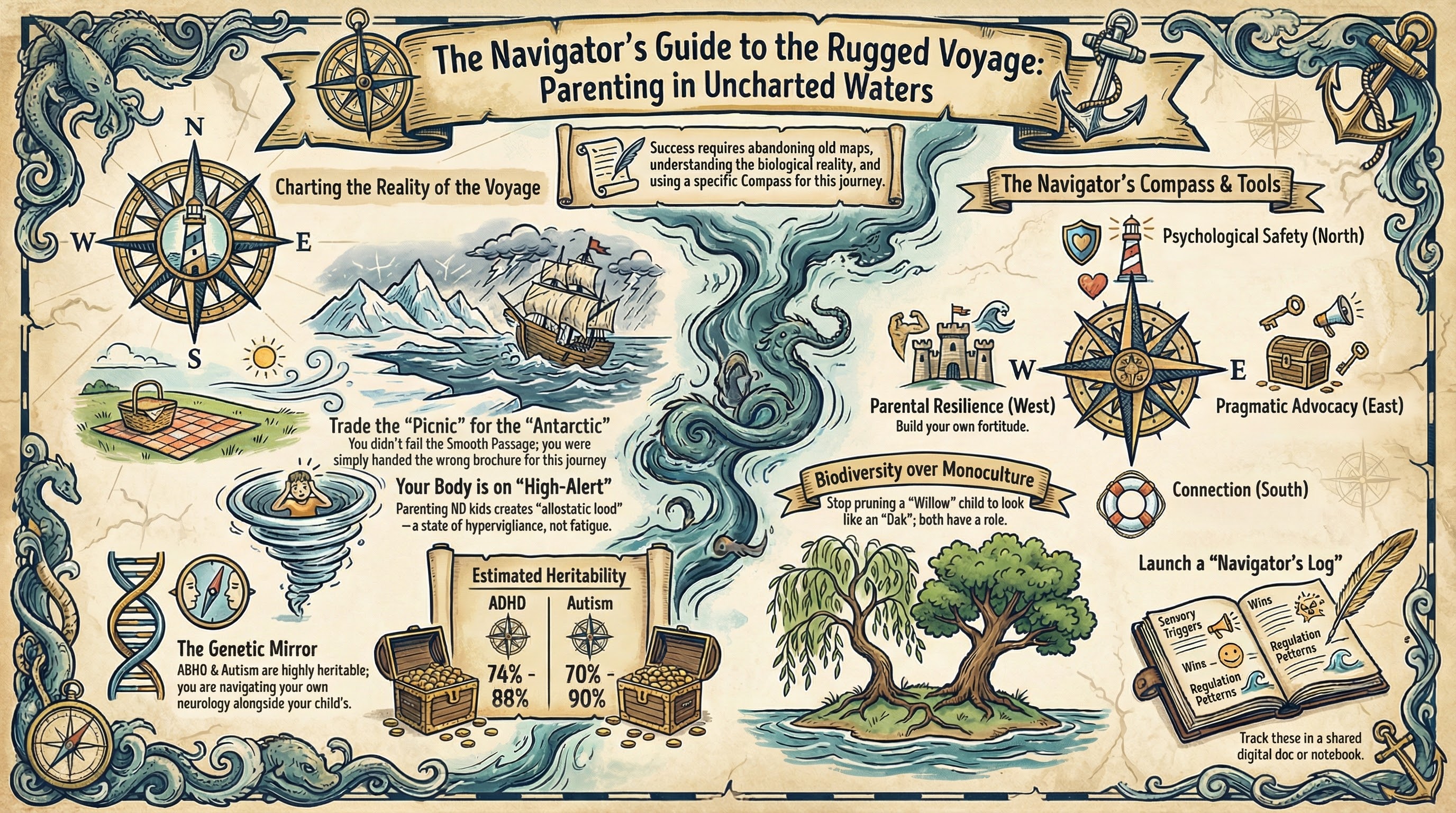

The Fusion Manifesto: We Draw Our Own Maps
We are the sailors who set out for a coastal sail and found ourselves in the ice-choked waters of an Antarctic passage. We packed for a picnic—snacks, a blanket, maybe sunscreen—only to discover the conditions required not just life vests and storm jibs, but ice axes and oxygen tanks. Equipment for a magnitude of voyage we never trained for. Gear whose weight we can still feel in our shoulders at the end of each day. If you have stood in your kitchen amidst the wreckage of a "rogue wave" morning routine, muscles trembling from holding a child through a meltdown, and thought This wasn't in the brochure, you are in the right place.
Standard parenting advice operates on a linear equation: consistency plus love equals a regulated child. For neurodivergent families, however, the math is non-Euclidean. Input A might yield Output Z, or Output Chaos. The maps handed down by neighbors or grandparents often lead us onto reefs. To survive, we must become cartographers. We must draw our own maps.
This book is a "Fusion Manifesto." It rejects the choice between clinical data and personal reality. We need both: the poetry to describe the storm and the meteorology to predict it. We need the anatomy to understand why a sock’s texture feels like a physical assault to a child’s nervous system.
Whether you are married and keeping your partnership afloat, or separated co-captains shouting across a chasm—a divide so deep you can barely see the other side—the mission is the same: safe passage for the child and sanity for the team. We are not here to turn the sea into a pond. We are here to learn seamanship.
The Myth of the Smooth Passage
Before we can plot a course, we must first mourn the map we lost. Almost every parent starts this voyage clutching a brochure for a different trip. We thought we were booking a "Smooth Passage"—a trip defined by milestones met on time, easy parent-teacher conferences, and the quiet satisfaction of a job well done. We expected the "Picnic."
When that reality dissolves, it is normal to feel not just fear, but grief. You may feel angry at the parents whose biggest problem is a child who won't eat broccoli, while you are managing violent meltdowns or navigating the labyrinth of special education law. You may feel a profound sense of "bait and switch." This anger is not a sign of bad parenting; it is a symptom of disorientation. You packed for Italy, and you landed in Holland (to borrow from Emily Perl Kingsley), but in our case, you packed for a Caribbean cruise and landed in the Drake Passage.
The danger lies not in the storm, but in the expectation of calm. If you believe the water should be flat, every wave feels like a failure. If you believe your child should be able to sit still at dinner, her movement feels like defiance. This gap between expectation and reality is where burnout breeds.
This book asks you to tear up the brochure for the Smooth Passage. It is a fiction that serves no one. Instead, we embrace the "Rugged Voyage." It is not a disaster — it is simply a sterner, more demanding kind of sea travel. It requires a sturdier vessel, a more skilled crew, and a deeper understanding of the elements. It offers views that the tourists on the cruise ship will never see—the bioluminescence of a unique mind, the raw beauty of unfiltered authenticity, and the profound strength that comes from weathering the gale. You are not a failed tourist; you are an elite mariner in training.
Quick Map: If you only read one page, read this
- The New Waters: You are a navigator in a parenting seascape that mainstream manuals don't cover.
- The Neurodiversity Paradigm: Differences in neurology are biodiversity, not just deficits.
- The Stress Reality: Parenting ND kids involves chronic hypervigilance; stress markers run high.
- The Mission: Success means becoming a cartographer of your child's unique brain.
- Shared Leadership: Alignment between co-parents is the primary "navigational aid."
Field Guide: The Science of Neurodivergent Parenting Stress
What's happening in the brain/body: Parenting a neurodivergent child creates chronic "allostatic load"—wear and tear from prolonged stress. Research shows parents of autistic and ADHD children report significantly higher stress compared to those with neurotypical children. Your system operates in hypervigilance: the amygdala (threat detector) stays activated, scanning for the next meltdown. Elevated cortisol becomes your baseline. This isn't "fatigue"—it's a physiological high-alert mode.
What it looks like at home: You wake up bracing for battle. You can't relax at a restaurant because you're scanning exit routes. Your heart races when the school calls. Even in calm moments, you're waiting for the other shoe to drop. Transitions trigger anxiety. Disagreements with co-parents feel like life-or-death conflicts because you're both depleted.
What helps:
- Name it: Recognizing this as a biological response (not weakness) reduces shame.
- Micro-rest: Steal 60-second resets (cold water on face, deep breaths).
- Shared language: Use neuroscience (dopamine, executive function) to turn arguments into collaboration.
- Lower the bar: "Good enough" is the goal. Frozen pizza is a tool, not a failure.
- Find your cohort: Other ND parents ("neuro-kin") provide vital validation.
What backfires:
- Comparing yourself to neurotypical parents—you're climbing a different mountain.
- Waiting for it to get easier before you rest—rest must happen during the voyage.
- Fighting your co-parent about strategies instead of testing approaches together.
- Hiding the struggle—isolation makes stress worse.
- Expecting the child to "just try harder"—willpower can't override neurology.
One sentence to remember: "You are not failing at normal parenting—you are succeeding at exceptional parenting under extraordinary conditions."
You Are Not Alone: The Statistics of the Voyage
The isolation of this voyage is its most dangerous feature. You might feel like the only parent whose child is screaming at the playground. It is easy to feel marooned. But the data reveals a crowded archipelago of families weathering the same gales.
Consider the "Miller" family (a composite of thousands of families). Sarah and Mark are sitting in their car after a school meeting. They are silent. The teacher just told them their 7-year-old, Chloe, flipped a desk. Again. Sarah is crying because she feels like a failure; Mark is angry because he feels judged. They go home to separate corners, too exhausted to comfort each other. This scene is playing out in driveways, kitchens, and therapist waiting rooms across the world right now. You are part of a vast, silent fleet.
Research validates the weight you feel. Raising an autistic or ADHD child involves much higher stress than raising neurotypical children.¹ Some parents show stress markers similar to those in high-conflict environments.² This isn't just a busy schedule; it's hypervigilance.
The strain on co-parenting is real. While "80% divorce rates" are an exaggeration, the risk is still elevated.³ Families managing ODD face even more friction. Chronic defiance and volatility can drain the emotional reserves needed for a healthy relationship.⁴
These numbers aren't here to scare you. They are here to validate you. If your relationship feels like it is fraying, it is because you are bearing a heavy load. You are navigating a high-stakes environment with fewer resources than you need. The Millers didn't fail because they didn't love Chloe; they struggled because they were trying to sail a hurricane in a dinghy. This book is about building a bigger boat.
Embracing Neurodiversity: Biodiversity of the Mind
To create a functional map, we must first accept the nature of the terrain. We are operating under the banner of Neurodiversity. This paradigm posits that neurological variations like ADHD, Autism, and Dyslexia are not errors in the human code, but natural variations—biodiversity of the human mind.⁵
Imagine a forest. A healthy ecosystem is not composed entirely of oak trees. It requires the deep roots of the oak, yes, but also the rapid growth of the pine, the flexibility of the willow, and the ground cover of the fern. Each plant has a specific role, a specific way of processing sunlight and water.
For a century, society has tried to farm humans like a monoculture of corn. We expected every child to grow in the same rows, at the same height, requiring the same amount of water. When a child grew differently—faster, slower, or sideways—we labeled them "disordered." We spent decades trying to prune the willow tree to look like an oak, and then wondered why the willow was stressed, broken, and failing to thrive.
The Neurodiversity paradigm asks us to stop monocropping our children. It challenges us to look at the child who cannot sit still and see a hunter-gatherer in a classroom designed for farmers. It asks us to look at the child who lines up cars and see a systemic thinker in a world that values social chaos.
Society has spent a century pathologizing these differences, framing them solely through the lens of deficit: Deficit of attention, disorder of social communication, defiant disorder. While we do not minimize the disability and struggle involved—these conditions can be profoundly disabling in a world not built for them—we must also recognize the inherent validity of these neurotypes.
- The ADHD Brain is a divergent thinking engine. It is capable of hyperfocus and creative leaps.
- The Autistic Mind often shows strengths in pattern recognition and detail-focused processing.⁶
- The PDA Profile is a fierce drive for autonomy. These are traits we celebrate in adult leaders but often punish in children.⁷
- The ODD Response is often a protective shield. It is a threat-detection system on high alert.⁴
Our job is not to "cure" our children. We cannot turn a willow tree into an oak. Our job is to create the conditions in which she can thrive. This requires looking in the mirror. ADHD and Autism are highly heritable.⁸ It is likely that one or both parents share these traits.
Understanding your own neurology allows you to navigate your child's map with empathy. Understanding your own "messiness" or "short fuse" as a trait, not a failing, is liberating.
The Four Cardinal Points of the Compass
Every navigator needs a compass. In the chaos of a diagnosis or a custody dispute, it is easy to spin in circles, reacting to the loudest crisis rather than steering toward a goal. Throughout this book, we will return to four fixed points that guide every decision, every interaction, and every strategy.
1. North: Psychological Safety (The Hull) Safety is not just the absence of physical danger; it is the presence of nervous system regulation. For a child with PDA, safety means autonomy. For an Autistic child, safety means predictability. For an ADHD child, safety means being accepted, impulse-warts and all. If the hull is breached (if the child feels unsafe, shamed, or terrified), the ship cannot sail. Every strategy we propose begins with the question: Does this make the child feel safe?
2. South: Connection (The Anchor) When the storm rages, connection is what holds the ship in place. It is easy to become a "Case Manager"—dispensing meds, driving to therapy, attending meetings—and forget to be a parent. Connection is the antidote to the trauma of correction. We will prioritize strategies that build the bond between parent and child, even when that bond is tested by ODD defiance or withdrawal.
3. East: Pragmatic Advocacy (The Radio) We cannot sail in silence. We must communicate with the other vessels in our vicinity—schools, doctors, therapists, and extended family. Advocacy is not about demanding special treatment; it is about translating your child’s coordinates to a world that doesn't speak their language. We will equip you with the scripts, the laws, and the confidence to broadcast your child’s needs clearly and effectively.
4. West: Parental Resilience (The Keel) The keel is the heavy, underwater fin that keeps a boat from tipping over in high winds. You are the keel. If you capsize, the whole family goes over. This book unapologetically prioritizes your mental health, your sleep, and your boundaries. We reject the myth of the martyr-parent. A depleted captain cannot steer a complex vessel. Taking care of yourself is not "me-time"; it is structural maintenance of the ship.
The Genetic Mirror: Looking at Your Own Map
Our job is not to "cure" our children. We cannot turn a willow tree into an oak. Our job is to create the conditions in which she can thrive. This requires looking in the mirror.
ADHD and Autism are highly heritable.⁸ The statistics are not abstract—they are deeply personal:
- ADHD heritability: 74-88%
- Autism heritability: 70-90%
If your child has ADHD, there is a statistically high probability that you do too—diagnosed or not. If your child is autistic, one or both parents likely share traits on the spectrum, even if you've spent decades masking them.
Understanding your own neurology allows you to navigate your child's map with empathy. Understanding your own "messiness" or "short fuse" as a trait, not a failing, is liberating.
But there's more to this than liberation. Your neurodivergence directly shapes your co-parenting dynamics. And until you name it, you will fight against it.
The Science Behind "It Runs in Families"
Perhaps you've pursued genetic testing for your child. Perhaps the results came back "negative" or "inconclusive." Perhaps you thought, "But I can SEE it runs in our family. How is the test negative?"
Here's why: The heritability is real, even when genetic tests don't confirm it.
Modern genetics distinguishes between "twin heritability" (how much genetics contributes overall) and "SNP heritability" (how much we can detect with current genetic tests). Twin studies consistently show ADHD is 74-88% heritable and autism is 70-90% heritable. But when researchers use genome-wide association studies (GWAS) to identify common genetic markers (SNPs), current technology can capture approximately 11-12% of the genetic variance for autism.
This is called the "Missing Heritability Paradox." But here's the crucial point: this lower number does not mean genetics "only matter 12%." It means current technology using common variants only captures a fraction of the genetic picture. The "missing" heritability isn't actually missing—it reflects technological limitations in detecting rare variants, structural variations, and complex gene interactions. The total genetic contribution (measured by twin studies) remains high.
Why the gap exists:
Rare Variants: Genetic changes present in less than 1% of the population have large effects but are hard to detect in aggregate studies. Your family's specific genetic cocktail may be unique.
Structural Variation: Copy Number Variants (CNVs)—deletions or duplications of DNA segments—are more common in neurodivergent individuals but aren't captured by standard tests.
Gene Interactions: Complex interactions between genes (epistasis) mean the effect of one gene depends on the presence of others. The "polygenic symphony" is more than the sum of its parts.
What this means for you: The scientific consensus confirms that neurodivergence is highly heritable even if specific genetic causes cannot be identified in a clinical setting. Negative genetic test results do not invalidate what you observe in your family tree. The genes are there; we just don't have the resolution to see all of them yet.
You are not imagining the inheritance. The mirror is reflecting biological reality.
The Cascade: How Diagnosis Reveals the Family Tree
Many parents discover their own neurodivergence through their child's diagnosis. It often unfolds as a cascade:
Stage 1: The Child's Diagnosis Your son or daughter is assessed. You sit in the psychologist's office, listening to the symptom list: impulsivity, time-blindness, sensory sensitivities, difficulty with transitions, emotional dysregulation.
You nod. You recognize these traits. You've been managing them in your child for years.
Stage 2: The Mirror Moment Then the psychologist asks about your childhood. "Were you a hyperactive kid? Did you struggle to sit still in class? Did loud noises bother you? Did you lose things constantly?"
And something cracks open. Wait. That's me.
The "perfectly normal hyperactive kid" you remember wasn't normal. The "bit weird, tried to ignore sensory issues" wasn't quirky—it was neurodivergent. The forgetfulness you've apologized for your whole life wasn't a character flaw—it was ADHD executive dysfunction.
You've been describing yourself in your child's symptom list.
Stage 3: The Retroactive Recognition You start seeing it everywhere. Your daughter—the one you thought was "just like you, clever and funny and a bit weird"—was neurodivergent all along. You missed it because she looked like you. You couldn't see her ADHD because you couldn't see your own.
You recognize it in your own parent. The dad who threw tools when frustrated (dysregulation). The mom who needed the house perfectly quiet (sensory sensitivity). The sibling who went through five jobs in two years (ADHD impulsivity, rejection sensitivity).
The diagnosis didn't create the neurodivergence. It revealed the family tree.
A Note on the Mother-Son Pattern
If you're a mother reading this, you may have noticed a specific pattern: Your son is diagnosed with ADHD or autism. As you learn about the condition, you realize, "I struggled with this my whole life. But I was never diagnosed. How did he get it so much worse?"
This is not random. There is a biological mechanism called the Female Protective Effect (FPE).
Research suggests that biological females may require a higher threshold of genetic liability to manifest clinical autism or ADHD than males. In other words, you may have needed to carry MORE genetic risk factors to show the same symptoms your son displays.
What this means:
- As an undiagnosed woman, you may carry a high genetic load—more rare variants, higher polygenic risk scores—but the FPE "protected" you from meeting diagnostic criteria in childhood.
- When you passed those genes to your son, he did not have the FPE. Without that protection, the same genetic load manifested more visibly.
- You were not "quirky" or "sensitive" or "anxious." You were neurodivergent all along. Your son's diagnosis revealed your own undiagnosed traits.
This is not a failure of parenting. This is sexually dimorphic genetic expression.
The "Lost Generation" of undiagnosed mothers is, in many cases, a generation of women who carried high genetic risk but were protected from diagnosis by biology—only to see that risk fully expressed in their sons. Understanding this pattern is not about blame. It's about recognizing that you inherited these traits, and you passed them on, and neither of those things is within your control.
The guilt you feel is not scientifically justified. The FPE explains why you and your son can both be neurodivergent, even if your presentations look wildly different.
Stage 4: The Defensive Co-Parent You try to share this revelation with your co-parent. "I think I have ADHD too. And maybe you do?"
They resist. Hard.
"It's not ADHD. It's just stress." "I don't need a label." "It's my childhood trauma, not a brain difference."
This resistance is not about you. It's self-protection. Accepting the diagnosis for your child means confronting it in themselves—and they're not ready. They've built an entire identity around being "normal" despite the executive function chaos, the sensory overwhelm, the emotional storms they've white-knuckled through.
Your child's diagnosis is a mirror they're not ready to look into.
Stage 5: The Ongoing Discovery For some parents, the cascade continues. You get diagnosed with ADHD, then start exploring autism. Or you're diagnosed autistic, then recognize the ADHD traits you'd attributed to "anxiety." Your co-parent, who insisted it was "just CPTSD," eventually gets assessed and realizes it was both—trauma layered on top of undiagnosed neurodivergence.
This is not "too late." This is exactly on time.
Late diagnosis is common, especially for:
- Women (who mask more effectively and present as "anxious" or "depressed" rather than "hyperactive")
- High-IQ individuals (who compensate with intelligence, hiding executive dysfunction)
- People of color (who are systematically under-diagnosed and misdiagnosed with conduct disorders)
- Adults over 30 (who grew up before ADHD/autism were widely recognized)
If you're reading this and thinking, "Wait, this is describing me," trust that instinct. You're not imagining it.
Why This Matters for Co-Parenting
Understanding your own neurodivergence is not a sidebar—it is foundational to effective co-parenting. Here's why:
1. The "Clash of Operating Systems" Makes Sense
If you are an ADHD parent co-parenting with an autistic ex-partner, your conflicts may not be about "who's right." They may be about two different nervous systems colliding.
You (ADHD):
- Thrive on novelty, spontaneity, last-minute changes
- Struggle with time-blindness (chronically late to handoffs)
- Hyperfocus on special interests, lose track of scheduled calls
- Interpret routine as "rigidity" or "control"
Them (Autistic):
- Need predictability, advance notice, detailed schedules
- Require sameness to feel regulated
- Interpret your lateness as "disrespect" or "not caring"
- Experience your spontaneity as chaos
Neither of you is wrong. You're running incompatible operating systems.
Once you name the dynamic—"This is ADHD time-blindness clashing with autistic need for predictability"—you stop blaming each other. You start scaffolding for the difference. You set alarms for yourself. They send you calendar invites with reminders. You agree that they'll handle scheduling, you'll handle crisis flexibility.
The conflict doesn't disappear, but the shame does.
2. The ADHD/ADHD Household Chaos
If both co-parents have ADHD, the household may descend into what one parent called "a beautiful disaster."
The Double Executive Function Deficit:
- Neither parent remembers to check if the other packed the school bag
- Both parents lose the custody schedule (it's in an email... somewhere)
- Morning handoffs happen 30 minutes late because both of you have time-blindness
- The child's medication runs out because neither parent refilled it on time
This isn't incompetence. This is two brains with executive dysfunction trying to be each other's external cortex. It doesn't work.
The Solution: Outsource your executive function to technology.
- Shared digital calendar with automated reminders (for BOTH parents)
- Medication tracker apps (Medisafe, Round Health) with alerts
- "Launch Pad" zones in BOTH homes (keys, bags, forms go HERE, always)
- Co-parenting apps (OurFamilyWizard) that send automatic alerts for missed communications
You're not accommodating "the ADHD parent"—you're accommodating BOTH of you.
3. The Sensory Mismatch Catastrophe
If one parent is autistic with auditory sensitivity and the other is ADHD with constant vocal stimming (humming, singing, talking to themselves), handoff time can become unbearable.
The Autistic Parent: The ADHD co-parent's constant noise feels like needles in the brain. By the time the child arrives (also vocal stimming), the autistic parent is already at sensory capacity. They snap. They seem "cold" or "mean." They retreat to a quiet room, and the child feels rejected.
The ADHD Parent: The autistic co-parent's need for silence feels like rejection. "Why can't they just talk to me normally? Why do they always leave?" The ADHD parent doesn't recognize it as sensory overload—they interpret it as emotional withdrawal.
The Solution: Name it. Accommodate it. Protect it.
- Autistic parent wears noise-canceling headphones during "witching hour" (the hour after child arrives when everyone is dysregulated)
- ADHD parent learns to recognize "I need quiet" as a sensory need, not personal rejection
- Child learns that "Dad needs his headphones" is not punishment—it's how his nervous system stays online
You stop taking it personally. You start accommodating each other's neurology the same way you accommodate the child's.
The Undiagnosed Parent: The Silent Saboteur
One of the most treacherous dynamics occurs when one parent is diagnosed (or suspects their neurodivergence) and the other remains undiagnosed—and defensive.
The Pattern:
- Parent A gets their child assessed for ADHD. The psychologist says, "This is clearly genetic. Do either of you have ADHD?"
- Parent A recognizes themselves immediately. "Oh my god. That's me."
- Parent B insists: "I'm fine. This is about the child, not me."
But Parent B is not fine. They are:
- Chronically late (time-blindness)
- Losing important documents (executive dysfunction)
- Snapping at minor frustrations (emotional dysregulation)
- Needing the house to be exactly the same way every time the child visits (autistic routine need)
But they cannot see it. Because seeing it means confronting decades of shame, failure, and "what's wrong with me?" They've built their identity around "I'm normal, just stressed/busy/overwhelmed."
Your child's diagnosis is a mirror. And they are not ready to look.
The Result:
- Parent B refuses to use ADHD-friendly co-parenting tools ("I don't need an app to remember things")
- Parent B blames Parent A for "making everything about diagnoses"
- Parent B denies the child's needs ("She's just being manipulative") because accepting them means accepting their own
- The co-parenting relationship fractures along a neurological fault line
What Helps:
- Do not argue the neuroscience yourself. You are the ex-spouse; your credibility is compromised. Bring them to the source—a joint appointment with the child's psychologist.
- Frame accommodations as "what works" rather than "because you have ADHD." ("Let's use a shared calendar because we both have crazy schedules" vs "You need this because you're ADHD.")
- Recognize that their resistance is grief. They are mourning the "normal" identity they worked so hard to maintain. Give them time. Some parents come around after years. Some never do.
If they never do, you proceed with parallel parenting. You cannot make them see themselves. But you can protect your child from being the battleground of their denial.
The Gift of the Double Map
Here is the radical reframe:
Understanding your neurodivergence makes you a BETTER parent to your neurodivergent child.
You stop fighting your own nature. You stop apologizing for your ADHD forgetfulness, your autistic need for sameness, your PDA resistance to authority. You start accommodating yourself—which models self-acceptance for your child.
When your daughter sees you using noise-canceling headphones, she learns that sensory protection is healthy, not shameful.
When your son sees you set five alarms for important appointments, he learns that external scaffolding is smart, not weak.
When your child hears you say, "I have ADHD too, and I forget things sometimes. That's why I use a calendar," they learn that neurodivergence is a reality to navigate, not a flaw to hide.
You become the guide who's walked the terrain, not the tour guide reading from a script.
You stop trying to be the neurotypical parent you were never going to be. You start designing a co-parenting structure that works with both your brains, not against them.
And your child—watching you accept yourself—learns that they are not broken.
They are neurodivergent. Just like you. And that is not a tragedy.
It is your family's operating system.
When You Don't See Yourself in Your Child
Perhaps you've read this entire section and thought, "But I DON'T see myself in my child. They're nothing like me. Their autism is severe. They're non-speaking. They have intellectual disability. I don't have any of that. Does that mean I didn't pass this down?"
This is a crucial distinction: Genetic does not always mean hereditary.
A significant proportion of neurodivergence—particularly autism with intellectual disability or complex medical needs—is caused by de novo mutations. These are spontaneous genetic errors that occur during reproduction and are NOT present in the parents' DNA.
What this means:
- Your child's neurodivergence can be genetic (biologically rooted in their DNA) WITHOUT being inherited from you.
- De novo mutations are "new" events. You didn't carry the gene; it spontaneously occurred in the egg or sperm that formed your child.
- This is especially common in the "Mixed ASD with Developmental Delay" subtype—children with severe presentations often carry spontaneous mutations, not familial transmission.
Why this matters:
If you're a parent who doesn't "see yourself" in your severely affected child, you are not imagining the difference. The genetic root cause may be distinct from your own neurology.
This does not diminish your role as their guide. Even if you don't share the exact neurological substrate, you are still navigating neurodivergent terrain together. Your job is not to "relate" through personal experience—it's to observe, learn, and accommodate what your child needs, even when it's foreign to your own experience.
The reframe: You are not "passing down a burden." In many cases, you are simply the parent of a child whose unique biology emerged spontaneously. Guilt over inheritance is scientifically unjustified in these cases.
Genetic root causes do not imply parental blame.
A Note for the Still-Discovering
If you are reading this section and thinking:
"I'm not sure if I'm neurodivergent. Maybe I'm just bad at organization. Maybe I'm just sensitive. Maybe I'm just making excuses."
Stop.
The fact that you are questioning whether your lifelong struggles "count" as neurodivergence is itself a symptom. Neurotypical people do not spend decades wondering why life feels harder for them than it looks for everyone else.
You do not need a formal diagnosis to use the accommodations in this book. You do not need a psychiatrist's letter to set alarms for your time-blindness, wear noise-canceling headphones for your sensory sensitivity, or use ADHD-friendly co-parenting apps.
But if you want to pursue assessment, know this:
Adult ADHD and autism diagnosis is valid, valuable, and common in parents of neurodivergent children.
You are not "faking it." You are not "too old" or "too functional" to qualify. The diagnostic criteria were written for children, and many adults—especially women, people of color, and high-masking individuals—were overlooked.
Assessment is not about collecting labels. It's about understanding your brain's operating manual. It's about accessing accommodations that make life livable. It's about finally having language for the invisible weight you've carried alone.
And it's about looking your child in the eye and saying:
"I see you. Because I am you."
The Weight of the Cargo: Acknowledging the Invisible Labor
Beyond the maps and the charts lies the physical reality of the voyage: the weight of the cargo you carry every day. In the neurotypical world, parenting is often described as a series of moments. In our world, it is a constant, shimmering state of high-alertness. It is the invisible labor of the "External Frontal Lobe."
You are the one who remembers that the blue socks are the only ones that don’t feel like "stabbing needles." You are the one who translates the child's silent retreat as a sensory shutdown rather than rudeness. You are the one who pre-games every grocery store trip with the tactical precision of a heist movie. This labor is exhausting because it is relentless. There is no "off-duty" when your brain is constantly scanning for the next sensory trigger or dopamine dip.
When you add the complexity of co-parenting to this load, the weight can feel crushing. Shouting across the channel between two households about medication timing or IEP goals isn't just a logistical challenge; it is a physiological drain. Every disagreement with your co-captain is a leak in the hull. Every moment of feeling judged by your partner is a headwind that slows the entire vessel.
We acknowledge this weight because if we don’t name it, we cannot manage it. You are not "stressed" because you are disorganized; you are burdened because you are performing a high-level cognitive and emotional service for another human being while simultaneously navigating a relationship that may be under repair. This book is your permission slip to acknowledge that the cargo is heavy. Our goal is to help you distribute that weight more effectively between the captains, so the ship sits higher in the water and sails with more grace.
How to Use This Book: Your Survival Kit
This book is not a novel to be read passively in bed (though you are welcome to do so). It is a field guide. It is designed to be dog-eared, highlighted, and argued over.
The Structure of the Voyage:
- Field Guide Sidebars: These sections break down the hard science—the "geology" of the brain. When we discuss a meltdown, we will pause to explain the amygdala hijack so you understand the biology of the scream.
- Parent Toolkit Exercises: At the end of chapters, you will find interactive prompts. You won't learn navigation only by reading about a compass; you have to pick one up. These exercises—mapping routines, scripting conflict, auditing sensory needs—transform theory into practice.
- Survival Tips: These are the emergency flares—quick, bulleted lists of strategies for the heat of the moment when your prefrontal cortex has gone offline.
The Navigator's Commitment: This is not a book of theory; it is a book of action. We ask you to make a contract with yourself today.
- I will stop waiting for "normal." I accept the voyage I am on.
- I will be curious, not critical. When my child (or my co-parent) struggles, I will ask "Why?" before I judge.
- I will put on my own oxygen mask. I recognize that my well-being is the single greatest predictor of my child's success.
We invite you to open a "Navigator's Log"—a notebook or a digital file—to track your findings. You are about to become the world's leading expert on your child. Let the voyage begin.
Parent Toolkit: The Navigator's Log Setup
The Navigator's Log is your personalised field guide to your child — a shared (or parallel) documentation system for tracking sensory profiles, regulation patterns, communication keys, wins, and medication notes across both households. Set it up in 10 minutes using a shared Google Doc, co-parenting app, or even voice memos, then review weekly for patterns invisible to the naked eye. If co-parents disagree on format or participation, each captain keeps their own log — one well-kept log is better than none.
→ Download the full printable toolkit at thiswasntinthebrochure.wtf/toolkit Available as a printable infographic (PNG) and slide deck (PDF/PPTX).
Survival Card: The Co-Parenting Compass
When you feel lost in a storm of blame, ego, or overwhelm, this card anchors you. It covers the essential DO/DON'T checklist for co-parenting conflict — checking your North Star ("Is this about my ego or the child's safety?"), using the Pause before reacting, and scripts for your co-parent and yourself. The repair step and self-regulation cue remind you: you cannot steer the ship if you are drowning.
→ Download the printable Survival Card at thiswasntinthebrochure.wtf/toolkit Available as a printable infographic (PNG) and slide deck (PDF/PPTX).
Works cited
- Stress Assessment in Parents of Children With Autism Spectrum Disorder: A Prospective Case-Control Study - PubMed, accessed on December 19, 2025, https://pubmed.ncbi.nlm.nih.gov/39473684/
- Autism and Maternal Stress | Psychology Today, accessed on December 19, 2025, https://www.psychologytoday.com/us/blog/the-flourishing-family/202109/autism-and-maternal-stress
- Autism and ADHD: A Literature Review Regarding Their Impacts on Parental Divorce - PMC, accessed on December 19, 2025, https://pmc.ncbi.nlm.nih.gov/articles/PMC10047374/
- Oppositional Defiance or Faulty Neuroception? - Dr. Mona Delahooke, accessed on December 19, 2025, https://monadelahooke.com/oppositional-defiance-faulty-neuroception/
- Neurodivergent Affirming Language Guide - Neurodiverse Connection, accessed on December 19, 2025, https://ndconnection.co.uk/resources/p/nd-affirming-language-guide
- Enhanced Perceptual Functioning in Autism: An Update, and Eight Principles of Autistic Perception - Journal of Autism and Developmental Disorders, 2006, https://doi.org/10.1007/s10803-005-0040-7
- Understanding Pathological Demand Avoidance: What It Is, Why It Happens, and How to Navigate It - Momwell, accessed on December 19, 2025, https://momwell.com/blog/understanding-pathological-demand-avoidance
- Autism Spectrum Disorder: Genetic Mechanisms and Inheritance Patterns - MDPI, accessed on December 19, 2025, https://www.mdpi.com/2073-4425/16/5/478